.avif)
Your referral sources are active. Your team is working hard. Your reputation is solid.
But your census hasn't moved in months.
If you're running a healthcare organization with under 100 employees, this scenario probably feels familiar. You've tried adjusting your outreach. You've followed up on referrals faster. You've even considered hiring a marketing agency.
The problem isn't your effort. It's your system.
Most healthcare operators assume stagnant census growth is a marketing problem. More visibility, more outreach, more referral relationships. But when you look at the data, the real issue becomes clear: you're losing patients you already have access to.
This article breaks down the structural gaps that keep healthcare organizations stuck at the same census level, why referral dependence creates unpredictable growth, and how to build an acquisition system that converts consistently.

The Hidden Cost of Referral Dependency
Referrals are valuable. They convert at an average of 7.2%, significantly higher than most marketing channels.
But here's what most operators miss: even strong referral sources leave 14-30% of potential patients on the table due to broken internal systems.
One children's hospital lifted patient referral conversion rates from 70% to 86% by fixing structural intake issues. They didn't generate more referrals. They stopped losing the ones they already had.
When you depend entirely on referrals, you're building growth on someone else's timeline. If a referral source changes their process, hires a new coordinator, or shifts their priorities, your census drops. You have no control.
The organizations that grow predictably don't abandon referrals. They build systems that convert referrals more effectively while adding direct patient acquisition channels they can measure and control.
Your Intake Process Is Probably Costing You Patients
Most healthcare organizations don't have an intake problem. They have a conversion problem disguised as an intake process.
Here's what the data shows:
It takes intake coordinators about 70 minutes to review a referral packet. That's plenty of time for potential patients to move on. About 30% of referrals are rejected because the patient's needs don't match the organization's offerings. The first to respond usually wins.
A home care agency implementing a new intake process saw a nearly 80% increase in admissions and a 60% improvement in their closing ratio within just 30 days. Another home health agency that often went months without admissions experienced a 100% increase in monthly admissions thirty days after revising its intake process.
The structural fix delivered immediate census growth without any marketing changes.
Your intake process should answer three questions immediately:
• Can we serve this patient?
• What's the next step?
• Who owns this conversion?
If your team has to hunt for answers, you're losing patients before they ever schedule.
The Real Cost of Slow Response
Patients who arrive on time still contribute to delays when intake forms occupy 10–15 minutes. That effectively makes on-time patients a quarter hour late for their actual appointment slot.
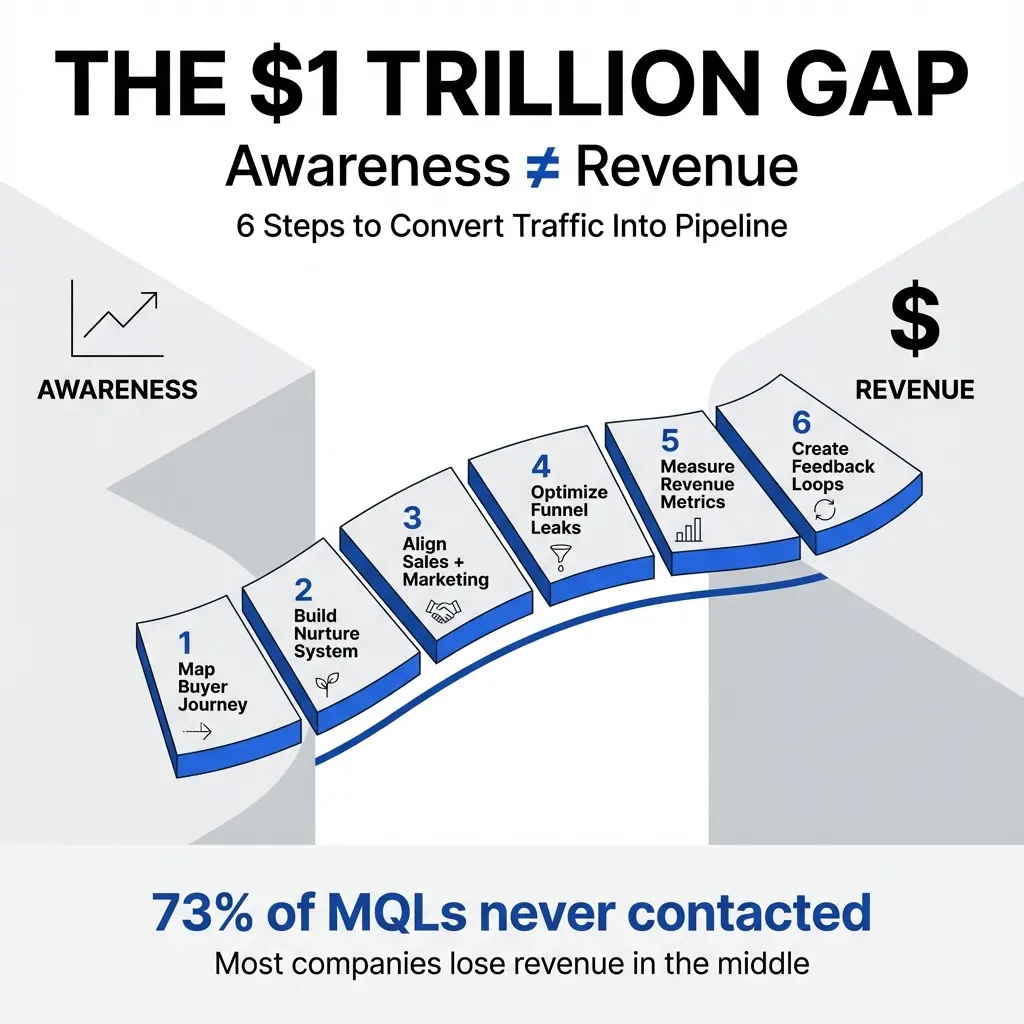
Nearly 30% of America's healthcare spending (over $1 trillion annually) goes toward administrative tasks. Manual, repetitive work leads to higher drop-offs, lower retention, more patient switching to other providers, increased staff burnout, and worse ROI.
Speed matters. But speed without clarity just creates faster confusion.
The Conversion Gap No One Talks About
The medical practitioners' industry median patient conversion rate is 3.6%. The average is 7.4%. Top performers convert up to 21%.
Top performers don't generate more traffic. They convert better through systems.
You can't optimize what you can't see. Most healthcare organizations under 100 employees don't have a clear view of their patient acquisition funnel. They know how many referrals they received. They know how many patients enrolled. Everything in between is a black box.
Here's what you need to track:
• How many inquiries you received (referrals, calls, form submissions)
• How many turned into scheduled consultations
• How many consultations happened
• How many consultations converted to admissions
When you map this out, you'll see where patients drop off. That's where you fix the system.
Why Patients Disappear After the First Contact
Among the primary causes of unfulfilled referrals: hospitals were only attempting two phone calls to referred families, and providers weren't able to schedule appointments directly.
Two attempts. Then the patient is gone.
People who miss even one appointment have a 70% dropout rate compared to 19% for those who show up regularly. One missed touchpoint equals lost census permanently.
Your conversion infrastructure needs to handle the reality that patients are busy, distracted, and evaluating multiple options. If your system assumes they'll respond on the first try, you're designing for failure.
The Financial Reality of Broken Systems
Patients miss 30% of scheduled appointments. The U.S. healthcare system loses about $150 billion yearly. Medical practices report average yearly losses of $22,872 from cancelations and no-shows.
Now add acquisition costs.
Average healthcare cost-per-click is $3.17. Average cost per lead is $162–$320. Paid digital leads can exceed $400 in competitive markets.
A patient who schedules a single consultation and never returns creates a net loss when you consider acquisition costs. Even patients who visit regularly may not bring in enough revenue to cover the initial investment if your conversion rate is below industry benchmarks.
Marketing without conversion infrastructure burns money.

How to Build an Acquisition System That Actually Works
Healthcare organizations rarely lack demand. Clinics, therapy practices, dental groups, and home health agencies often face more referrals than they can absorb.
Yet expansion frequently stalls. Rapid growth can introduce instability that erodes margin, quality, or reputation.
The organizations that scale predictably don't just add more marketing. They build acquisition systems that handle increased volume without breaking.
Step 1: Map Your Current Patient Journey
Start by documenting every step a patient takes from first contact to admission. Include:
• How they find you (referral, search, direct call)
• What happens when they make contact
• Who responds and how quickly
• What information they receive
• How scheduling happens
• What happens between scheduling and the appointment
• What happens after the first visit
You'll find gaps immediately. Most healthcare organizations discover they have no consistent process for follow-up, no clear ownership of conversion steps, and no way to measure where patients drop off.
Step 2: Fix Your Intake Process First
Your intake process should be fast, clear, and designed to qualify patients before they reach your clinical team.
Create a simple intake qualification checklist:
• Does this patient match our service offerings?
• Do we have capacity?
• What's the next step?
• Who owns this conversion?
Assign clear ownership. If no one owns the conversion, no one converts.
Step 3: Build a Follow-Up System That Persists
Two phone calls aren't enough. Build a follow-up sequence that includes:
• Immediate confirmation (text or email)
• Reminder 48 hours before the appointment
• Reminder 24 hours before the appointment
• Follow-up if they miss the appointment
This isn't aggressive. It's respectful of the reality that people forget, get busy, and need reminders.
Step 4: Track Conversion at Every Stage
You can't improve what you don't measure. Track:
• Inquiry-to-scheduled rate
• Scheduled-to-show rate
• Show-to-admission rate
• Overall inquiry-to-admission rate
When you have this data, you'll know exactly where to focus. If your inquiry-to-scheduled rate is low, your intake process needs work. If your scheduled-to-show rate is low, your follow-up system is broken. If your show-to-admission rate is low, your clinical team needs better conversion training.
Step 5: Add Predictable Demand Channels
Once your conversion infrastructure works, add channels you can control:
• Search visibility for high-intent queries
• Direct outreach to potential referral sources
• Patient education content that builds trust before the first call
These channels don't replace referrals. They reduce your dependence on any single source and give you predictable volume you can measure and optimize.
What This Looks Like in Practice
A home health agency we worked with was stuck at 45 active patients. They had strong referral relationships. Their clinical team was excellent. But census wouldn't move.
We mapped their patient journey and found the problem immediately: they had no follow-up system. If a referred patient didn't answer the first call, the intake coordinator moved on.
We built a simple follow-up sequence. Three calls over five days. A text message with scheduling options. An email with service details.
Within 30 days, their inquiry-to-admission rate increased from 22% to 41%. They didn't get more referrals. They stopped losing the ones they already had.
Six months later, they were at 72 active patients. Same referral sources. Same team size. Different system.
The Next Step
If your census is flat, the problem probably isn't your marketing. It's your system.
You're losing patients you already have access to because your intake process is slow, your follow-up is inconsistent, or you can't see where conversions break down.
Fixing this doesn't require a bigger team or a massive budget. It requires clarity about where patients drop off and a system that converts consistently.
About the Author







.svg)
.svg)





.png)























.png)






















.png)

.jpg)





.jpg)



